Yes, COVID Vaccines Do Slow Transmission
Here’s our sad state of affairs: actual science lost the information war about four years ago. That’s when well funded anti-vaxxers and wellness grifters started flooding social media with biased medical information via cherry-picked studies, deliberately misinterpreted statements from health officials, and miscommunication of complex scientific data.
One of the now ubiquitous (false) beliefs is that COVID vaccines do not slow disease transmission. They absolutely do. They once did so very well, and now not so well, unless you recently got a booster and that booster was well matched to the circulating strain.
To lay out the evidence for this, I created a Twitter thread back in 2024. (Yes, it’s Twitter. I refuse to refer to that cesspool of bots and ideology by the beautiful 25th letter of the English alphabet. Best I can do is xitter.)
These data are not controversial among scientists. And yet somehow they have been forgotten and ignored by the zeitgeist. Let’s break them down in a way that I hope most people can digest and appreciate…
What Do We Expect the Vaccines to Do?
To begin, let’s remember that vaccines seek to do four things, in descending order of importance and likelihood:
A. prevent death
B. prevent hospitalization
C. prevent symptomatic disease
D. prevent infection & transmission
Transmission reduction is the product of (a) being less likely to get infected, and (b) being less likely to pass something on if infected. If you think about it, these are difficult things to measure, which is why a single randomized controlled trial (RCT) is often insufficient. To do this properly, you need long term surveillance programs and invasive testing capacity to measure what we call “secondary attack rates” or SARs.
But I’m getting ahead of myself…
What Did the Initial COVID mRNA Vaccine Do?
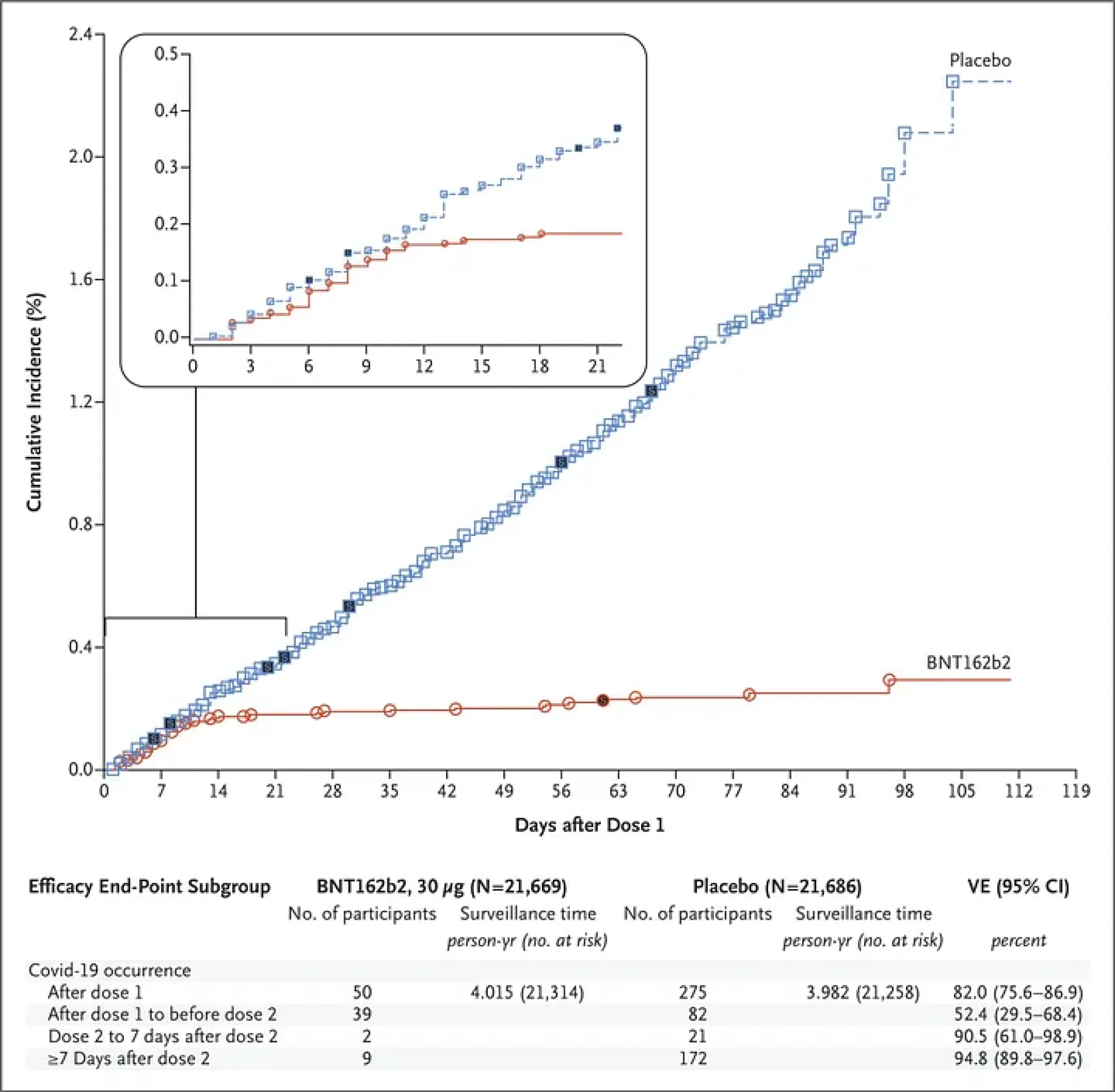
In an historic, triumphant publication, Pfizer’s COVID mRNA vaccine was shown in the first pivotal RCT to be 94.8 per cent effective in preventing symptomatic disease caused by original Wuhan variant, or wild-type strain.
This early efficacy graph is so statistically awesome that it caused many jaws to drop. I still show it to my students as an example of what science can do when well-funded and deemed urgent. It is one of the most scrutinized graphs in human history, and I (and others) did many media interviews in December of 2020 explaining its every nuance:
The later follow-up curve for the efficacy on kids aged 5–11 is equally impressive. So much so that I had it emblazoned on a variety of products!
A 94.8 per cent efficacy against symptomatic disease is awesome. But it’s not technically a 94.8 per cent protection against infection or transmission. Though it’s close. If you prevent symptoms, you go a long way toward preventing transmission, even in a disease known for its asymptomatic spread.
Now, to receive Emergency Use Authorization, the vaccine did NOT need to stop transmission (though that would have been nice). The actual criterion was reduction in symptomatic disease by >50 per cent, which was met and exceeded, as we see in the figure.
It is important to underline again that this initial pivotal RCT did not provide evidence that the vaccine stopped or slowed transmission, only that it was highly highly likely to prevent symptomatic disease. Those are not the same things (the difference between goal C and goal D above.) I took great pains to express this to the media at the time. The reasons that this was not explored in this study are many, but include that that was not what the US federal government had asked for. They’d asked for something that could prevent disease and not necessarily infection, and that’s what they got.
The goal, remember, was to stop this disease from filling the hospitals, killing people, and stopping society. That’s actually an easier goal to achieve than stopping transmission.
Even so, there was a strong suspicion that this vaccine would slow transmission. Why? Because when you prevent symptomatic disease for a respiratory infection like this, you also prevent the primary means of transmission (i.e., people sneezing and coughing in your face.) But, again, this RCT did not offer overt evidence to that end.
But It DID Slow Transmission
Although this is not what the government asked for, those original COVID vaccine formulations (Pfizer, Moderna, AstraZeneca, etc) DID reduce transmission, as shown in multiple studies in early 2021.
For example, Pfizer’s own investigation found that transmission was reduced significantly after only one dose. And, more rigorously, an Israeli study found that the vaccine reduced susceptibility to infection (likelihood of getting infected) by 89.4 per cent while infectiousness (likelihood of spreading infection) was a mere 23 per cent, leading to a combined efficacy against transmission of 91.8 per cent. That’s an awesome statistic!
There were multiple studies in 2021 that confirmed the same thing: COVID vaccination reduced disease transmission by a lot.
Then Came Vaccine Passports
This was when some countries brought in vaccine passports, which made scientific sense at the time, given the strong signal that transmission was being curtailed.
Now, if you want to debate the ethics of those passports, please do so elsewhere. There is ripe opportunity to explore the tension between rights curtailment and social good. It’s great fodder for civics and philosophy forums. But none of that has anything to do with the fact that the vaccines were totally reducing transmission.
Societies at that time desperately needed more people to get vaccinated faster before (here comes the foreshadowing) vaccine resistant variants could emerge. The intent of the passports -whether you agree with them or not- was to allow for faster re-openings of businesses while also incentivizing more people to get vaccinated.
The data for this were compelling. By slowing mixing of vaccinated & unvaccinated populations, the risk of breakthrough infections was reduced.
And that’s another thing the lay public is confused about. If the vaccines work, why do breakthrough infections happen? Well, in short, it’s because 91.8 per cent efficacy is not 100 per cent efficacy. That 8.2 per cent gap is going to express itself if there’s enough exposure happening…. which is why public health was eager to get a lot more people vaccinated: so that exposure would become less likely!
It’s like wearing high rain boots to keep your feet dry when the streets are flooded. They work great until the floodwaters are over your knees.
Enter Delta
The emergence of the Delta variant changed the math considerably. Two doses of vaccine were still ~70 per cent effective at preventing Delta infection, which was pretty darned good! We could have still tamed the pandemic with vaccination if we did it fast enough…
Now hear this in Morgan Freeman’s narrator voice: “They did not, in fact, vaccinate fast enough.”
Enter Omicron
The emergence of the Omicron variant in late 2021 changed everything by noticeably curtailing vaccine efficacy. This is when vaccine passports stopped making scientific sense and when herd immunity became mathematically out of reach.
See, the passports were now disproportionately exposing vaccinated people to the virus, since they were the only ones allowed to be out in society. But those same vaccinated people had diminished protection due to the rise of Omicron. The unvaccinated, denied entry to public places, were not as exposed. So for a brief moment in December of 2021, in some places the vaccinated were seeing a higher rate of infection than the unvaccinated.
This data blip is regularly accentuated and amplified by antivaxxers as proof that the vaccine “causes” COVID. It does not. This is an example of selection bias, a statistical error that in this case gives the illusion that one group is more susceptible than another; but it’s actually because one group is more exposed (or “selected”) than the other. I hope you get that.
Rigorous studies, like this one published this year, have found that though Omicron really reduced the vaccine’s ability to curtail COVID's spread, you were still much better off being vaccinated than unvaccinated.
(As an aside, they also found that if you were really well vaccinated, then an infection afterwards offered considerable additional protection against reinfection later. So vaccination was supercharging “naturally acquired” immunity while reducing the negative impacts of that infection).
Here’s a quick visual appraisal, from the now defunct Ontario COVID-19 science advisory table:
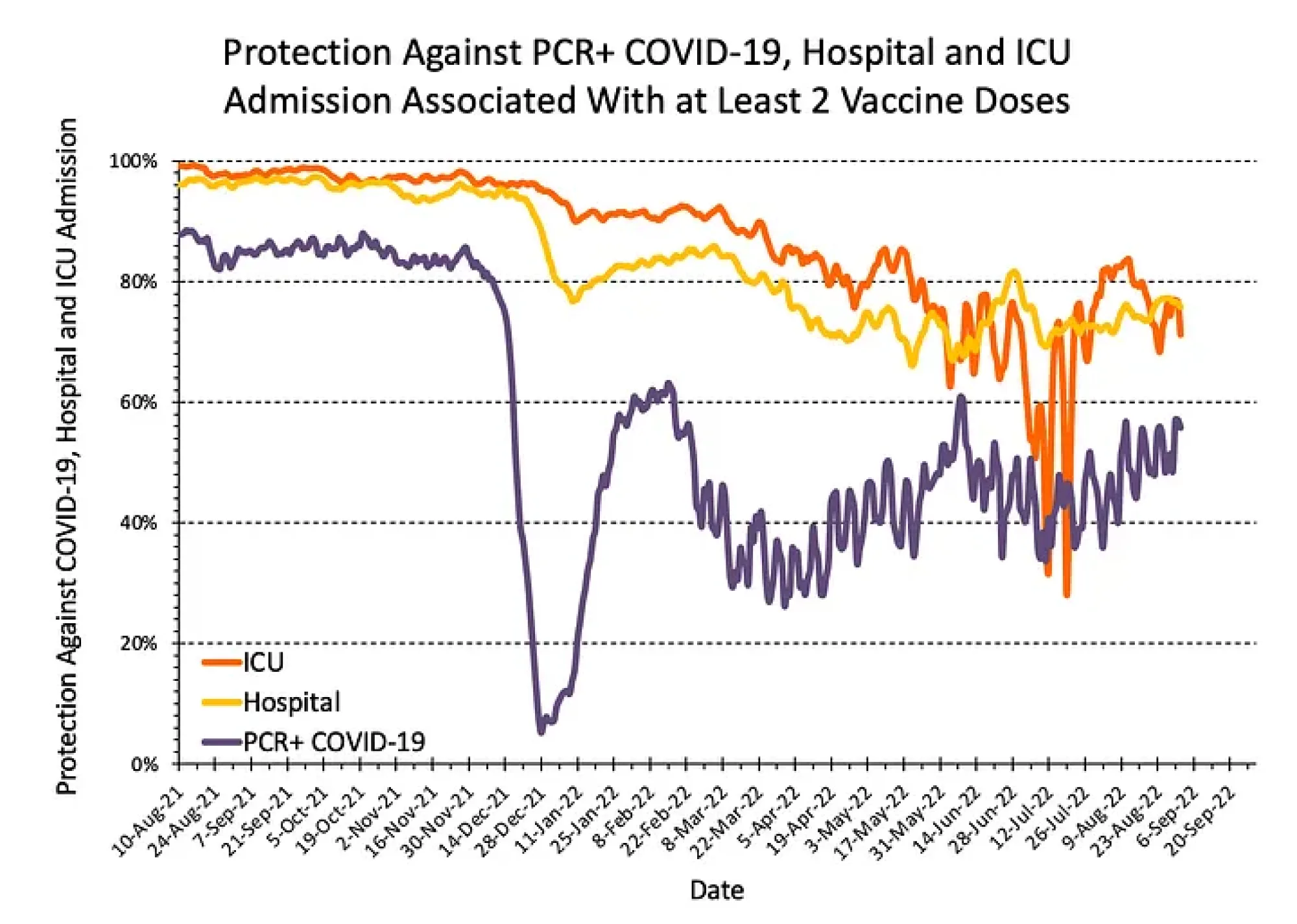
You can see from the graph that well into 2022 (when Omicron had established dominance), two doses of vaccine were close to 80 per cent effective at keeping you out of the hospital, and around 50 per cent effective and preventing you from being infected in the first place.
That very noticeable dip in December of 2021? Well, that was the vaccine passport selection bias I talked about above. See how dramatic it was? The passports were lifted immediately after that, the selection bias was taken away, and the true power of vaccination to stop infection was once again observable in the data.
The Omicron Years
By the end of 2022, it was clear that vaccination was no longer subduing transmission *significantly* (depending on how you define significantly). But three doses gave substantial protection against death for both delta (80 per cent) and omicron (78 per cent, along with 61 per cent protection against admission to hospital).
So beware the narrative of the vaccine minimizers. The original vaccine could still reduce Omicron transmission somewhat. This study estimated that any COVID vaccination was reducing Omicron transmission by at least 22 per cent. That ain’t nothing.
A telling California prison study found that one dose of any COVID vaccine reduced the probability of an infected inmate transmitting infection to his cellmate by 24 per cent. Again, that’s reduced transmission.
Subsequent Boosters
The so-called bivalent booster came out in Sep/2022. These were able to prevent actual infection by an impressive ~54 per cent, which means they were also significantly slowing transmission. But uptake was poor.
The XBB1.5 booster came out in 2023. It had an efficacy against hospitalization of >70 per cent, and also an efficacy of ~54 per cent against symptomatic infection. This is not as great as the 95 per cent we saw in 2020, but it’s pretty damned good! Only about 16 per cent of Canadians received this vaccine.
Data for more recent boosters is scarce.
What’s the Pattern?
UK surveillance suggests that every COVID booster results in a substantial (but not complete) reduction in onward transmission for several months, with the effect shrinking by 3–6 months.
Recall that transmission-reduction is the product of (a) being less likely to get infected and (b) being less likely to pass it on when infected. The pattern seems to be that each booster gives us a ~45 per cent reduction in infectiousness, together with ~30–55 per cent short-term protection against infection. At the population level, this translates to a likely drop in transmission from a recently boosted person of ~50–70 per cent in the first 1–2 months, fading thereafter.
But does this protection drop to nothing? Nope. Not at all.
This fantastic 2022 study did a global analysis of COVID vaccines’ various efficacies against transmission.
The research found that protection against transmission drops as new variants emerge and as time goes by since you got your shot. But it doesn’t drop to zero. And each booster spikes the protection up again.
TLDR:
Yes, COVID vaccines reduce transmission of COVID. Of course they do.
No, they don’t do so 100 per cent. But they once came close.
They reduce transmission best when: (a) the current booster is best matched to the circulating strain, and (b) people actually get the current booster.
So, please stop believing and spreading the outright lie that COVID vaccines do not slow transmission. They absolutely do. And if more people got them, there would be a lot less transmission and sickness in your community. Not zero, but a lot less.
---
Dr. Raywat Deonandan is a Global Health Epidemiologist and Professor at the University of Ottawa. He is a former Chief Scientist with the Canadian federal government, and an award-winning writer. Contrary to accusations from bots on X, he doesn't receive cheques from Klaus Schwab, Pfizer, or Bill Gates. Though that would be nice.
Another version of this article was originally published at https://blog.deonandan.com.








