
It's Canada’s ‘brain gain’ moment — if we don’t flub it
“We don’t want to miss this window,” says Dr. Joss Reimer, president of the Canadian Medical Association.
She says in the face of the chaos unfolding to the south, it would be a "small silver lining to have Canada gain a tremendous amount of medical and scientific expertise."
Over the past six months, the Medical Council of Canada has seen a twelve-fold increase in U.S. doctors initiating the licensing process. Nova Scotia is already onboarding its first cohort. Saskatchewan is advertising directly to American physicians, and Manitoba is preparing its own campaign.
Canada, it seems, has a historic opportunity. The question is: will Ottawa take it?
“The immigration system is not fast, and it’s not efficient,” says Alex Munter, the CMA’s newly appointed CEO and former head of Children’s Hospital of Eastern Ontario.
Munter says when he was at CHEO, it wasn’t unusual for it to take years to bring a physician into the country.
One physician who recently made the move from the U.S. to Canada had much to say about the roadblocks he faced in the resettlement process.
He spoke anonymously, fearing reprisal from figures in the U.S. Canada Healthwatch has verified his identity.
He says the U.S. government could make it "very difficult" for physicians to leave for Canada, should the mood strike. And he wonders if the opportunity to recruit them at scale may be time-limited.
He began the immigration process immediately after last year’s U.S. presidential election. After “a lot of fees” and time spent "filling out forms and making tons of phone calls,” he began working in a B.C. emergency room — five months later.
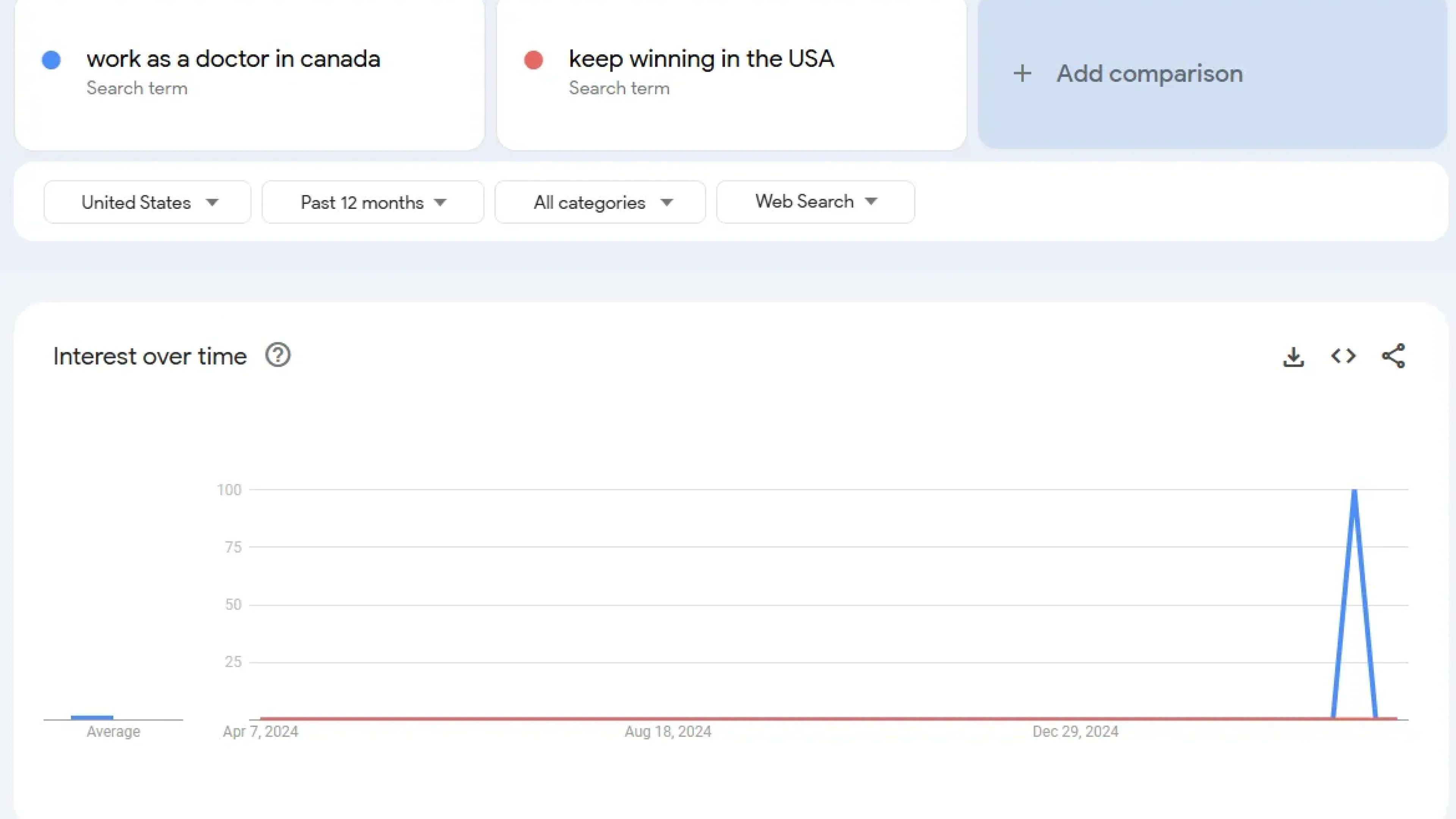
Google search interest in “work as a doctor in Canada” spiked last month, as disillusionment spreads south of the border.
He says representatives from the Medical Council of Canada, provincial colleges, hospital associations, and government ministries (among others) “need to work together in a single office,” to drastically reduce the paperwork and administrative burden involved in making the move.
“This would be probably the only thing that would facilitate [B.C. Health Minister Josie] Osborne’s goal of licensure in six weeks,” he says.
“To get a SIN you need a bank account. But even after I got one I couldn’t get my SIN.
I handled it. But it was just dumb.”
This bureaucratic gauntlet is exactly what the CMA is hoping to eliminate. Munter says Ottawa already has the tools it needs.
“The Minister of Immigration has the authority to create special pathways,” he says, pointing to efforts to expedite immigration for Ukrainians, and previously, Afghans.
“We need the federal government to be helping from the immigration side,” Reimer says. “Health Canada’s own report said we’re 23,000 family physicians short.”
Munter also points to the federal requirement for Labour Market Impact Assessments — a lengthy step in which hospitals must demonstrate that they tried to hire within Canada first.
Munter, Reimer, and the CMA are calling for two specific federal actions:
- A dedicated immigration pathway to accommodate physicians fleeing the U.S.
- An exemption on Labour Market Impact Assessments for physician jobs
Munter says two ministries — Immigration, and Jobs and Families (formerly Labour) — will both be needed to achieve these objectives. Until then, he says, things at the federal level are too cumbersome to fully realize the brain gain.

‘Bed blockers’ or abandoned patients? Inside Ontario’s push to discharge its most vulnerable
Ontario’s Bill 7 allows hospitals to fine patients who refuse discharge to long-term care. But documents show many of these so-called 'bed blockers' have nowhere else to go.
Why it's important: These people aren’t stuck in the hospital by choice. They’re left there by a system not built with their existence in mind.
Internal notes from Trillium Health Partners detail cases of patients with feeding tubes, gaping wounds, cognitive decline, or complex psychiatric needs — too complex for long-term care, too poor for private options. Patient advocates say the Ford government’s pressure to discharge “bed-blockers” shifts blame from its own systemic underinvestment to vulnerable patients. Some are fined thousands, despite having no money and nowhere to go.
Read more…

Trump order reaches north as Canadian researchers drop inclusive language
A leading Canadian research group is stripping gender-inclusive terms from U.S.-funded cancer trials, citing compliance with a Trump executive order.
Why it’s important: Political interference from the U.S. is shaping how science is conducted in Canada — even when it contradicts our own research standards.
Canadian Cancer Trials Group is removing terms from its studies including “gender” and “intersex” to keep its place in the U.S. National Cancer Institute’s trial network. The move has sparked alarm among scientists. “This is a moment to stand up for what’s right,” says bioethicist Françoise Baylis, a bioethicist. “If you acquiesce, you are, in fact, undermining trust in science.”
Read more…

Competition Bureau targets Express Scripts over alleged anti-competitive practices
Canada’s largest pharmacy benefit manager is under investigation for practices that critics say restrict patient choice and threaten independent pharmacies.
Why it’s important: The case could reshape the power dynamics in Canada’s pharmacy sector — and restore control to patients and providers.
The federal Competition Bureau is probing Express Scripts Canada over fees, audits, and alleged “patient steering” toward affiliated pharmacies. Pharmacists say the PBM’s dominance squeezes competitors and compromises care. Regulators will examine whether its practices amount to abuse of market power under the Competition Act. A decision here could set major precedent for the entire insurance sector in Canada.
Read more…
Carney hedges on privatization in Alberta health care debate
Liberal Leader Mark Carney drew some fire this week for giving a vague response when asked how he'd defend public healthcare.
Why it’s important: With Alberta heading into a privatization freefall, federal enforcement of the Canada Health Act is becoming a more important issue than federal parties are likely used to — and comfortable with.
Asked in Calgary how he’d respond to provinces expanding for-profit care, Carney emphasized “working with provinces” but avoided addressing enforcement of the Canada Health Act. Critics, including the Canadian Health Coalition and the NDP, called his answer evasive and inadequate. After securing the Liberal leadership one month ago, Carney said in his victory speech, “In America, healthcare is a big business. In Canada, it is a right,” to raucous applause.
Read more…








