COVID's long-term cardiac risk rivals that of diabetes: study
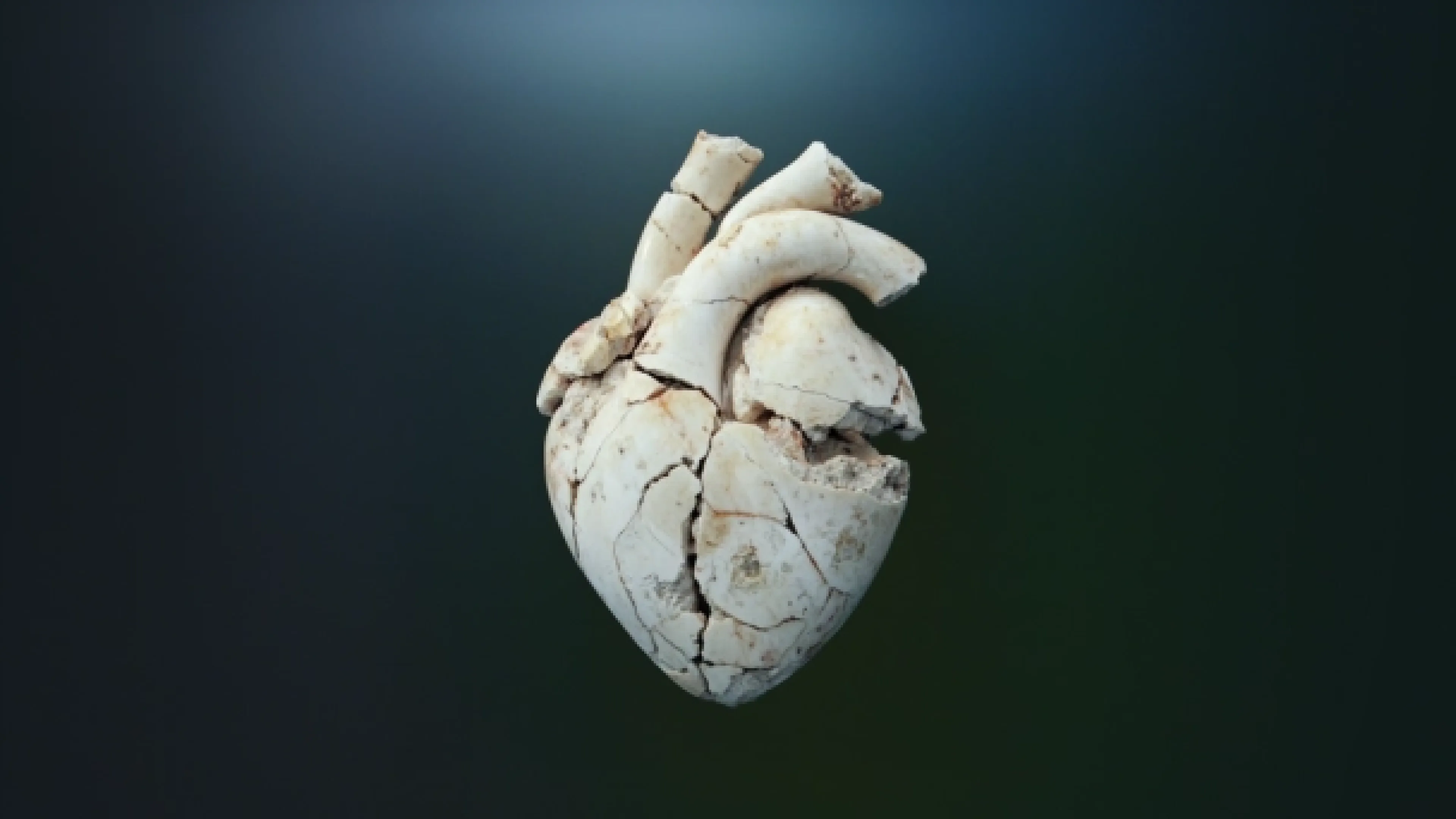
New research suggests COVID can double the risk of heart attacks and strokes for years after infection.
Why it's important: This week, CNN reported on a study of over 250,000 patient records showing increased risk of major thrombotic events for at least three years after a COVID infection.
Unlike other infections where heart attack risk subsides fairly quickly, these effects appear uniquely persistent. Acute COVID is also linked to a 1.5 times higher risk of car crashes (comparable to driving drunk) with no protective effect from vaccination. Evidence suggests that to reduce these population health impacts, at some point the airborne nature of transmission needs to be addressed.
Read more…
Quebec considers limiting family doctors to ‘vulnerable’ patients only
Quebec is exploring a model that would reserve family doctors for vulnerable patients, such as those with chronic illnesses.
Why it's important: The key question here is who decides which patients are “vulnerable?” After all, a healthy patient will stay "healthy" for as long as they go undiagnosed.
Quebec’s Health Minister, Christian Dubé, suggests prioritizing family doctors for high-need patients could improve care for those at risk. Critics warn the approach would lead to crowded ERs and less preventive care. The policy would be in keeping with Quebec’s apparent propensity to divert resources away from its youngest cohorts.
Read more…
Holland confident on Pharmacare deals by spring, despite Alberta pushback

Federal Health Minister Mark Holland says federal-provincial pharmacare agreements should be in place by spring.
Why it's important: Following this week’s passage of Bill C-64, The federal government can now negotiate with provinces to fund universal access to contraceptives and diabetes medications. While Holland is optimistic, Alberta isn’t.
Alberta Health Minister Adriana LaGrange is advocating for federal funds to enhance Alberta’s existing programs, while Federal Conservative Leader Pierre Poilievre said this week the bill threatens private drug plans. I expect the feds to move very quickly on this.
Read more…
Are Canada’s clinical trial participants being paid to stay quiet?
Some clinical trial participants are concealing side effects to complete studies and collect payments — risking their health and the integrity of drug research.
Why it's important: Participants, often economically vulnerable, face significant health risks as they bend rules to earn a living. The dynamic compromises the accuracy of trial data used to approve new drugs.
Canada’s clinical trial sector leads the G7 in trials per capita, but lacks the national monitoring systems of peer jurisdictions. Without stronger regulations, participants’ welfare and public safety are at risk.
Read more…
Harris wants seniors’ home-care covered by Medicare
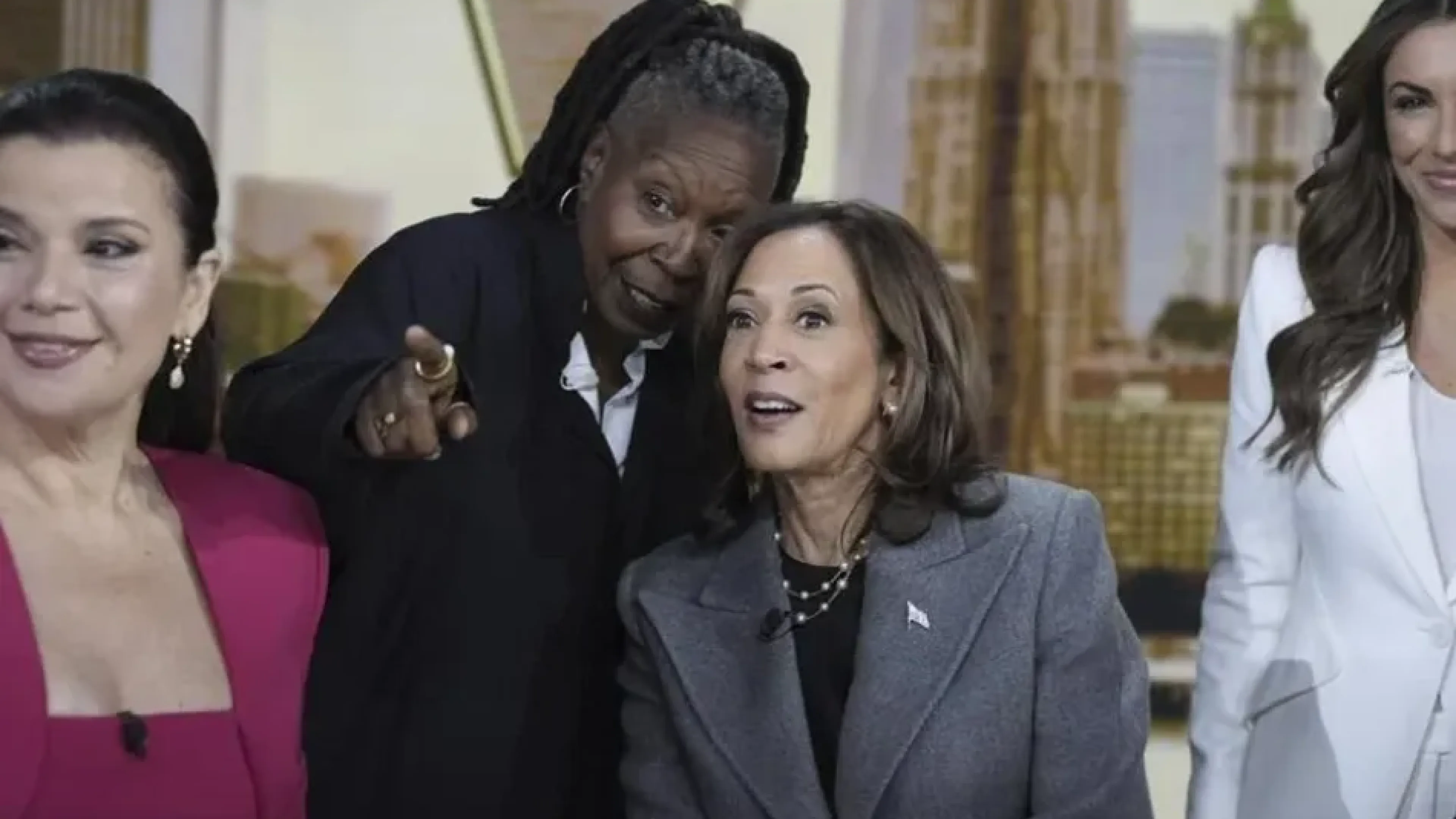
Kamala Harris plans to expand Medicare to cover in-home care for seniors, aiming to support Americans caring for aging parents and their own children.
Why it's important: While Canada has some provincial supports in-place to cover home-care, we have nothing approaching the comprehensiveness of what Harris is describing. We may see echoes of her proposal in the coming months and years.
The burden on Millennials and Gen X-ers caring for elderly parents creates a cycle of worsening economic impacts (or an economic death-spiral, if you will). As the sandwich generation is forced to opt out of the workforce to avoid the financial devastation of elder care, the tax base is further depleted in an already struggling economy. These effects disproportionately apply to women.
Read more…
French company set to disrupt Canada’s health insurance, virtual care markets

French health insurer Alan SA is entering Canada, offering group benefits and virtual health services, but the move raises concerns over potential limits on patient choice.
Why it’s important: Alan’s approach of combining insurance with virtual health services could challenge Canada’s major insurers, though it mirrors recent controversy over insurer-provider exclusivity deals.
Alan, valued at €4 billion, promises that Canadian employees will not be restricted to its app’s services and can choose any provider. But the broader trend of “payvider” models (where insurers provide health services directly) has some worried over the potential for patient steering, either through app-design or financial disincentives to seek care “out of network.”
Read more…








