Hello Healthwatchers! 👩⚕️👨⚕️
Welcome to this week’s edition. If there’s a theme to today’s newsletter, it’s “obscure stories you might have missed that are actually a pretty big deal.” Let’s get them on your radar.
Breast cancer screening sparks unexpected controversy
New guidelines from the Canadian Task Force on Preventive Health Care maintain that routine breast cancer screening should begin at age 50, despite public pressure and growing evidence that supports lowering the starting age to 40.
Why it's important: Critics, including prominent organizations and physician experts, say the decision ignores studies showing benefit to earlier screening and could endanger women's health by delaying detection of cancers, particularly in marginalized communities.
Health Minister Mark Holland expressed disappointment with the decision and announced an external review of the Task Force, while acknowledging that the body should continue to make science-based decisions that are arms-length from the whims of government. While Holland’s concerns are very much in-line with experts who say the guidelines are out of step with modern standards, his approach may set precedent for future health ministers to interfere with scientific advisory bodies.
Read more…
Health Minister defends new powers to pull products from shelves

Mark Holland deflected criticism of new rules allowing federal health ministers to pull health products from the market under certain circumstances.
Why it's important: Holland again! His new ministerial powers are a direct response to the misuse of nicotine pouches, which, though approved as aids to quit smoking, have been widely marketed to youth, potentially hooking a new generation of nicotine addicts.
Critics from industry-affiliated groups argue that such powers could lead to overreach from future health ministers, potentially affecting Canadians’ access to other products, like contraceptives — it’s a salient but cynical argument. Holland brushed off the claims as tobacco industry tactics to dilute public health measures, emphasizing that only a severe and blatant misuse of the new ministerial power would lead to such scenarios. The group levying the criticism, the Consumer Choice Center, receives funding from the libertarian think tank the Atlas network, as well as from Big Tobacco.
Read more…
Manitoba doctor expelled, censured for faking cancer

Monica Kehar, a former medical resident, claimed to have cancer to borrow over $160,000 from a colleague. Despite her expulsion from residency and censure by the College of Physicians and Surgeons of Manitoba, she continues to identify as a doctor while running a new business in B.C.
Why it's important: We may have a problem with the way we regulate medical titles. Canadian law allows anyone with a medical degree to use the title "doctor" even if they aren’t licensed to practice medicine.
Timothy Caulfield — my favourite expert on the topic of health misinformation — argues that the dilution of the doctor moniker is often misleading and in some scenarios, dangerous. Something else that’s not lost on me here is that my own title of 'Registered Nurse' is much more tightly regulated in most jurisdictions.
Read more…
Liberal health critic pushes for Ontario ban on private-pay NP clinics
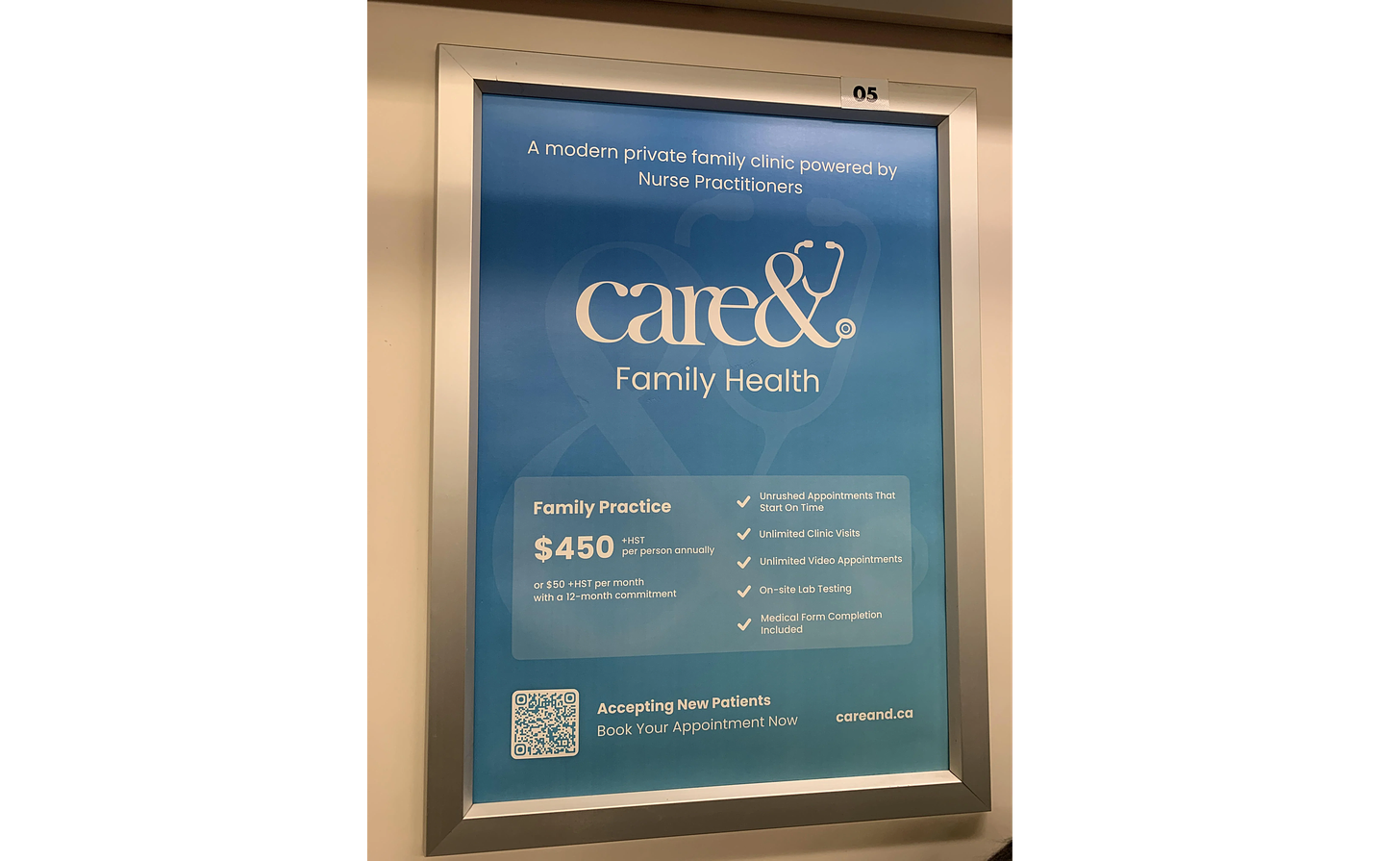
Ontario Liberal MPP Adil Shamji is set to introduce a bill to ban private-pay nurse practitioner clinics. The bill, if it were to pass, would also issue penalties for violations.
Why it's important: The proposed legislation aims to close loopholes allowing for private payments for primary care services covered under provincial health insurance.
The bill isn’t likely to pass, but if the Ontario Liberals were to take government in the coming years, this signals the direction they’re likely to take on this issue — if the governing PCs don’t beat them to the punch and close the loophole first. Shamji’s stance poses a direct contrast to the Ford government's current approach, for now. With at least 25 private clinics operating and more sure to open, the bill is timely and will probably see more attention from the public and legislators in the months ahead.
Read more…
Canadian scientists launch independent surveillance network to spot H5N1 in milk

Canadian researchers have initiated the Pan-Canadian Milk Network to monitor retail milk for traces of H5N1, aiming to enhance early detection and response to a potential outbreak of bird flu in Canadian livestock.
Why it's important: A good news story! This is a very prudent measure to stay on top of H5N1 as it continues to spread in U.S. dairy herds. This work could prevent significant disruptions to Canadian agriculture in addition to protecting public health.
Despite no current detections, the system offers a key layer of surveillance, complementing government efforts. The group includes some big names (including some you might recognize) and is posting the results of their work on a pre-print server, which I’ll be following. The U.S and other countries are now considering vaccination campaigns for farm workers, and it seems Moderna is a strong contender to be first out of the gate with an approved human mRNA vaccine.
Read more…
Experts urge disaster-proofing of hospitals against extreme climate events

Experts call for urgent measures to fortify Canadian hospitals against increasing climate-related disasters, stressing the need for resilient infrastructure to handle fires, floods, and extreme weather.
Why it's important: With climate-related emergencies on the rise, Canada's hospitals face some significant risks. Experts argue that we need enhanced ventilation, refurbished electrical systems, and air conditioning to protect our hospitals.
These steps, though costly, are essential to prevent much greater downstream expenses as well as loss of life. The CMA makes a compelling point: many of the country’s health facilities are over 50 years old and they’re among the oldest public infrastructure still in use today. Given their age and critical role, these facilities are especially vulnerable — disasters that typically bring people to ERs often affect the hospitals themselves.
Read more…
And that's it for this week, Healthwatchers.
These seemingly small stories have big implications, and I hope they've got your wheels turning. As always, your feedback is invaluable—I love hearing from our readers—so do drop me a line if something caught your eye this week.
Yours in health,
Nick Tsergas
National Health News Editor
Canada Healthwatch
[email protected] | canadahealthwatch.ca